
By: Shawna Fleming, MSc., BCBA & Brittany Clark, M.S., CCC-SLP
Interprofessional collaboration involves using the strengths of each profession to design a treatment approach that is effective and founded upon the best available research. It involves creating an environment that is based on shared values while fostering an inclusive team culture. While interprofessional collaboration has been associated with a number of benefits for clients and clinicians, it is often easier said than done. The relationship between Speech-Language Pathologists (SLPs) and Board Certified Behavior Analysts (BCBAs) has been particularly contentious. Generally speaking, there appears to be a fear of encroachment, stereotyping, and a lack of understanding about relative scopes of practice between the two professions.
As a BCBA in Ontario, Canada, Shawna has spent the last 6 years supervising ABA services for children with Autism Spectrum Disorder (ASD). Through her work with children with ASD, she’s had the opportunity to work with many professionals from other disciplines to collaborate and understand how our fields can work together to create positive outcomes. One of the professionals Shawna has had the opportunity to work with is Brittany Clark. Brittany is an SLP in Ontario, who has spent over 10 years working with individuals with developmental and acquired disabilities across the lifespan. It was through our collaborative work with children that we began to understand and appreciate the strengths of our respective disciplines. Brittany was the program director for community aphasia programs for many years, where she facilitated conversation groups and provided therapy to adults with aphasia. Our shared mentor, Tracie Lindblad, a dually certified SLP-BCBA, had a vision for an interdisciplinary intensive treatment program for adults with aphasia. Tracie suggested that we read A Behavioral Conceptualization of Aphasia (2008) by Baker, Leblanc and Raetz which provided a new way to look at treatment using a behavior-analytic lens. After reviewing the article, we were committed to making this happen! We were able to further our collaborative work by applying the science and research of both of our disciplines to rehabilitation therapy for adults post-stroke and designed a behaviourally-oriented intensive communication therapy for aphasia (BICA) program.
Aphasia is an acquired communication disorder, often caused from a stroke or brain injury, that impacts a person’s ability to speak, read, write and understand language. Despite aphasia being more prevalent than cerebral palsy, multiple sclerosis and Parkinson’s disease, very few people know about the disorder, and therefore do not understand the significant impact it has on a person’s quality of life. Intensive therapy has been shown to be effective for individuals with aphasia, but there are only about 18 intensive aphasia programs in the world, and none that use the science of behaviour analysis in their approach.
The intensive aphasia programs that exist are facilitated by SLPs and supportive personnel and follow a linguistic interpretation of language and communication. Traditionally, a linguistic interpretation of aphasia describes the individual’s deficits as being in either oral or written language, and either in expression or understanding. For individuals with aphasia, it is often not the entire receptive or expressive repertoire that is impacted (e.g. can respond to an intraverbal question about an item but cannot tact the item). Therefore, using the expressive/receptive dichotomy to assess and treat aphasia symptoms does not account for all aspects of the person’s language profile. Given that aphasia is an idiosyncratic condition, using the verbal operants to define communication provides a more accurate description of the person’s communication profile. Further, the use of stimulus control transfer procedures, systematic teaching, and ongoing data analysis are critical components of any intensive therapy program.
Prior to starting the intensive aphasia program, Shawna participated in community conversation groups facilitated by Brittany to better understand aphasia and the impact it has on a person’s life. We worked together to develop the structure of the intensive program by reviewing aphasiology research; Brittany had an understanding of effective interventions in aphasia rehabilitation and was able to guide Shawna through the various evidence-based practices for aphasia. Shawna was then able to reinterpret them using a behaviour analytic lens and create systematic teaching and data collection procedures. For example, Copy and Recall Treatment (CART) is a common therapy approach utilized by SLPs where a word is presented textually to the individual, the individual is asked to copy the word three times and then the model is removed, and they are asked to write out that word one more time (transcription task). In behaviour analysis, we would refer to this as a copy-to-transcription procedure and can then gradually and systematically fade out the prompt until the individual is able to transcribe the word independently.
Another aspect that we both vividly remember talking about was how we were going to use reinforcement to increase behaviour; in the intensive autism world, we typically use token boards or breaks with preferred items or activities, but we imagined that this approach wouldn’t be appropriate given we were working with adults. We decided that aside from providing praise, we could capitalize on the client’s motivation to make improvements and include the client in the data collection and graphing so that they could see the progress for themselves. This has been a very successful part of the program and helps the client see the benefits of their hard work! We continue to adapt our approach using the client’s motivation and values as our guide.
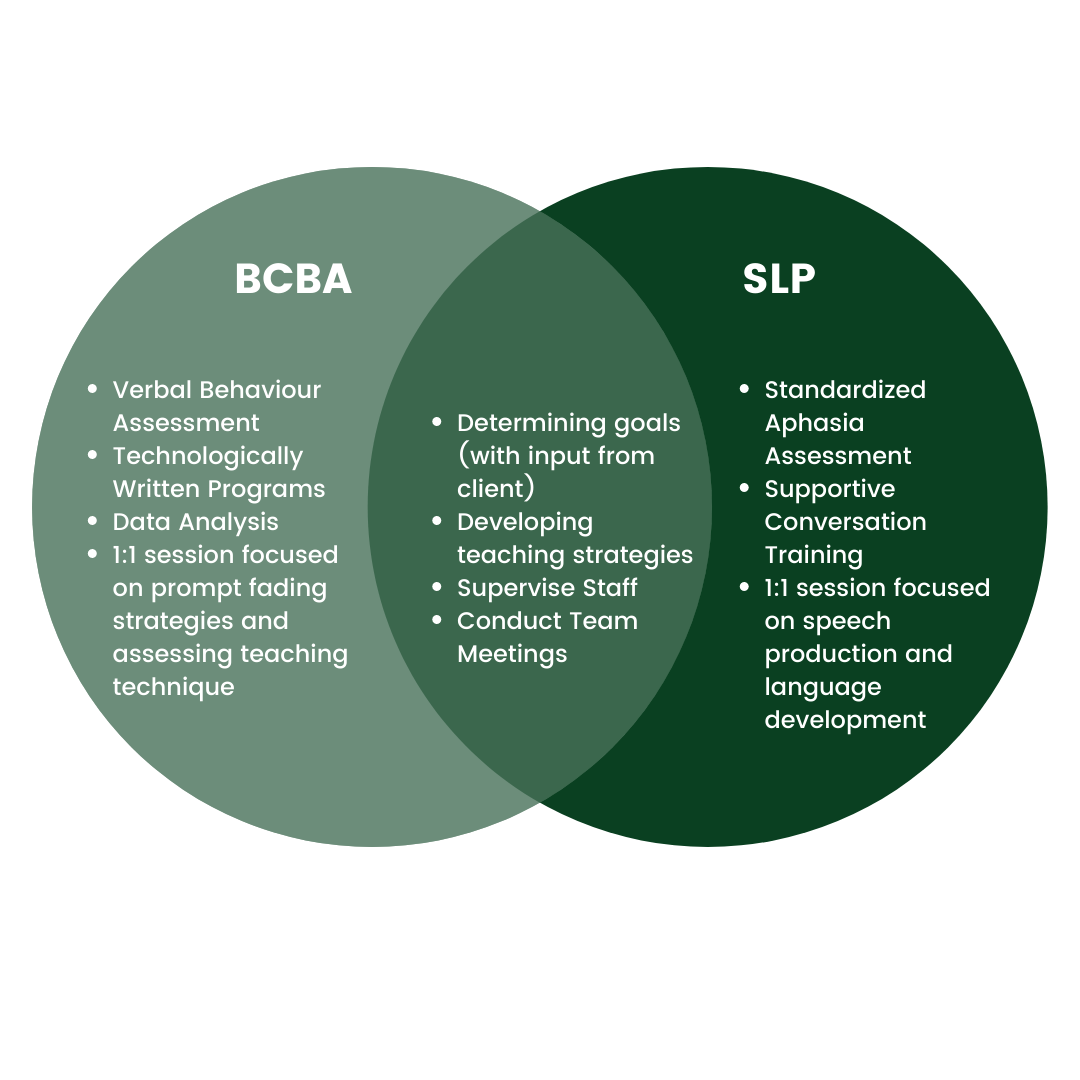
When the first couple of clients came through the program, Shawna observed Brittany conducting standardized assessments with the individuals. We would then work together to identify areas for treatment and develop teaching strategies. As the individuals participated in the program, Brittany observed and supervised the supportive personnel administering the program and conducted 1:1 sessions with the clients. Shawna would also observe the supportive personnel to assess treatment fidelity and would conduct data analysis weekly to flag programs for review. The model is not all that dissimilar from the intensive treatment we provide to children with autism, we are able to combine our knowledge of best practices to create individualized curriculums for our clients focused on creating functional improvements in their everyday life.
Evergreen Communication Therapy was established in 2021 by Brittany and Shawna to focus on interdisciplinary treatment of complex communication disorders. The intensive aphasia program at Evergreen is a 12-week program, consisting of 12 hours per week. During the first week of the program, the SLP conducts and interprets standardized assessments to determine baseline scores and abilities, the Behaviour Analyst interprets the assessments and further assesses skills across verbal operants, and together they develop an individualized curriculum targeting functional goals. The following weeks are primarily administered by supportive personnel (e.g. Communicative Disorder Assistants and Behaviour Technicians), with the SLP and BCBA both providing 1-hour of direct therapy per week, supervision, and team meetings.
Interprofessional collaboration can improve client outcomes and advance our understanding of complex disorders. At Evergreen, we see the value of interdisciplinary practice every day in the outcomes from our clients. We continue to learn and grow together, and are all better clinicians because of it!
References:
Baker, J. C., Leblanc, L. A., & Raetz, P. B. (2008). A behavioral conceptualization of aphasia. The Analysis of verbal behavior, 24(1), 147–158. https://doi.org/10.1007/BF03393063
Sidman, M. The behavioral analysis of aphasia. Neuropsychologia. 1971;8(413–422).
Comments are closed